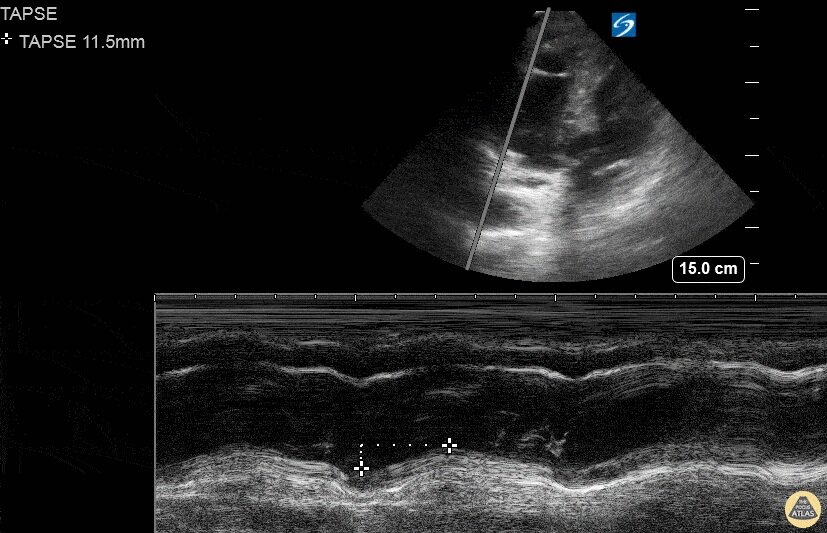
Middle age F presented initially to ED after a mechanical fall complaining of hip pain. Patient became tachypnic and altered during ER stay. POCUS done, and RA thrombus was noted with D sign and enlarged R ventricle.
R heart thrombus (thrombus in transit) is highly mobile differentiating it from a mural thrombus, which forms in situ. A meta-analysis of 1113 patients from the International Cooperative Pulmonary Embolism Registry showed mortality was 2x as high for pts with right heart thrombus and PE compared to those without right heart thrombus. The difference in mortality was more pronounced in the heparin alone treatment group (vs. lytics or embolectomy).
Another study by Rose et al (2002) showed patients with PE and a right heart thrombus had a mortality of 27%. They found these patients did better when treated more aggressively (i.e. thrombolysis or embolectomy).
Rose PS, Punjabi NM, Pearse DB. Treatment of right heart thromboemboli. Chest. 2002;121(3):806-14. (PMID: 11888964)
Torbicki A, Galié N, Covezzoli A, et al. Right heart thrombi in pulmonary embolism: results from the International Cooperative Pulmonary Embolism Registry. J Am Coll Cardiol. 2003;41(12):2245-51. (PMID: 12821255)
Submitted by Bobak Zonnoor, MD