Forearm Nerve Blocks
The median, radial, and ulnar nerve blocks allow anesthesia of the forearm and hand. The superficial position of these nerves and low anesthetic volume required makes blockade relatively straightforward. These blocks can be performed at the level of the upper arm, proximal to the elbow, or at the level of the forearm just proximal to the wrist.
Median Nerve Block
Indications: hand/wrist procedures, lacerations, and deep abscesses


Considerations & Technical Details
Considerations:
As the median nerve runs with the brachial artery, a negative aspiration prior to injection is essential to avoid inadvertent intravascular injection.
Needle: 25-27g 1-1.5 in (2.5-3.8 cm) needle
Anesthetic Volume: 4-5 mL
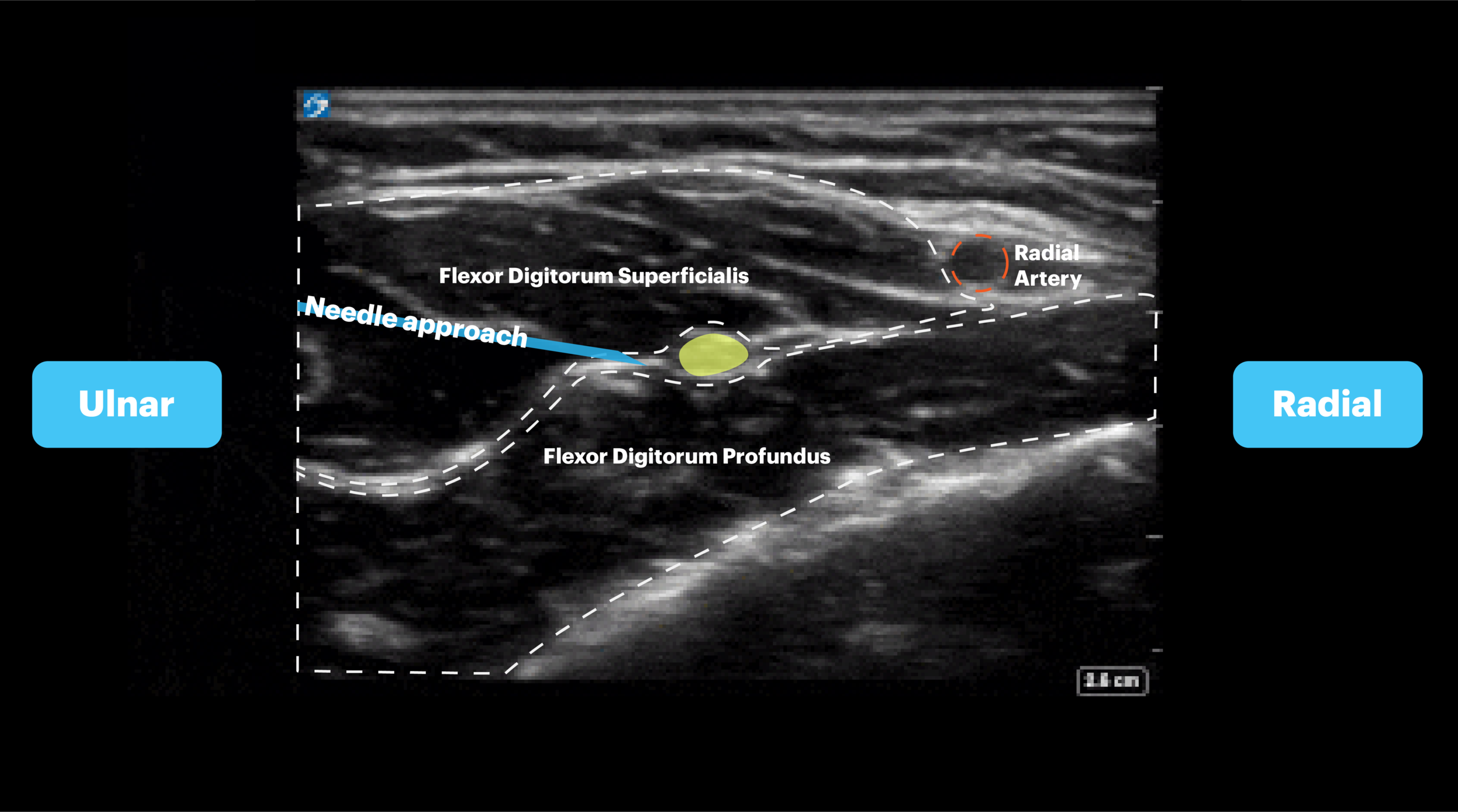
Target of Anesthetic: Anesthetic spread around the median nerve, along the fascial plane between the flexor digitorum superficialis (FDS) and the flexor digitorum profundus (FDP)
Positioning
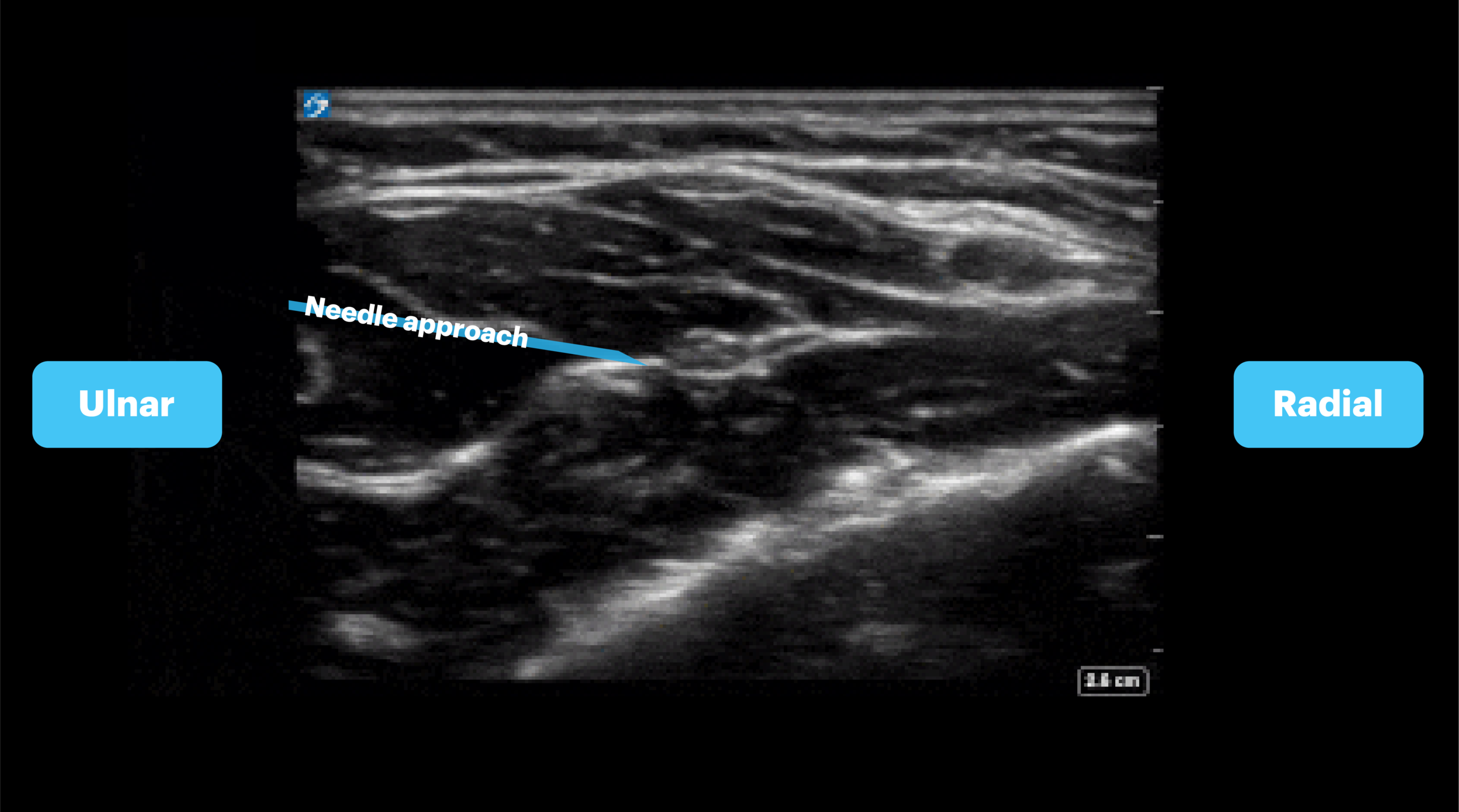
Position the patient supine with arm abducted from the patient exposing the volar forearm. Place the probe in transverse orientation over the midpoint of the forearm. The hyperechoic structure found in the fascial plane between the flexor digitorum superficialis and flexor digitorum profundus muscles is the median nerve.
Target Identification
This nerve is generally the easiest of the forearm nerves to find. Simply place the probe transverse, a few centimeters proximal to the wrist crease, and slide the probe proximally looking for the hyperechoic structure sandwiched between the two digital flexors muscles. Sometimes the nerve can be confused with the flexor tendons if you are too close the wrist so if you are unsure continue to slide towards mid forearm. The tendons will disappear while the median nerve will remain.

Needle Approach
There are multiple approaches to perform a median nerve block both in-plane and out-of-plane. Our preferred approach is an in-plane technique from the ulnar aspect of the arm. Once this view is obtained, the needle should be advanced from ulnar to radial towards the hyperechoic fascia between the flexor digitorum superficialis and flexor digitorum profundus. Notice that you are not aiming to hit the nerve but rather you are aiming to get just adjacent to the nerve within the fascial plane.
Median Nerve Blocks
Radial Nerve Block
Indications: hand/wrist procedures, lacerations, and deep abscesses

Considerations & Technical Details
Considerations:
If performed above the elbow, recall that the radial nerve contains both sensory and motor nerves, and blockade will result in a wrist drop.
Transducer: High-frequency linear probe
Needle: 25-27g 1-1.5 in (2.5-3.8 cm) needle
Anesthetic Volume: 4-5 mL
Target of Anesthetic: Within the fascial plane surrounding the radial nerve; specific anatomic location will vary based on forearm or above elbow block (see below)

Positioning - Wrist
With the forearm supinated, the transducer will eventually lie in a transverse orientation around 5-10 cm from the wrist crease.
Target Identification
The best way to identify the radial nerve is to start at the wrist. Place the probe in a transverse orientation, along the radial aspect of the volar wrist surface, a few centimeters proximal to the wrist crease. Identify the pulsatile radial artery, the radial nerve lies just radial to this. At this point it is too close to the artery to block so slide the probe proximally until the hyperechoic radial nerve can be seen splitting away.
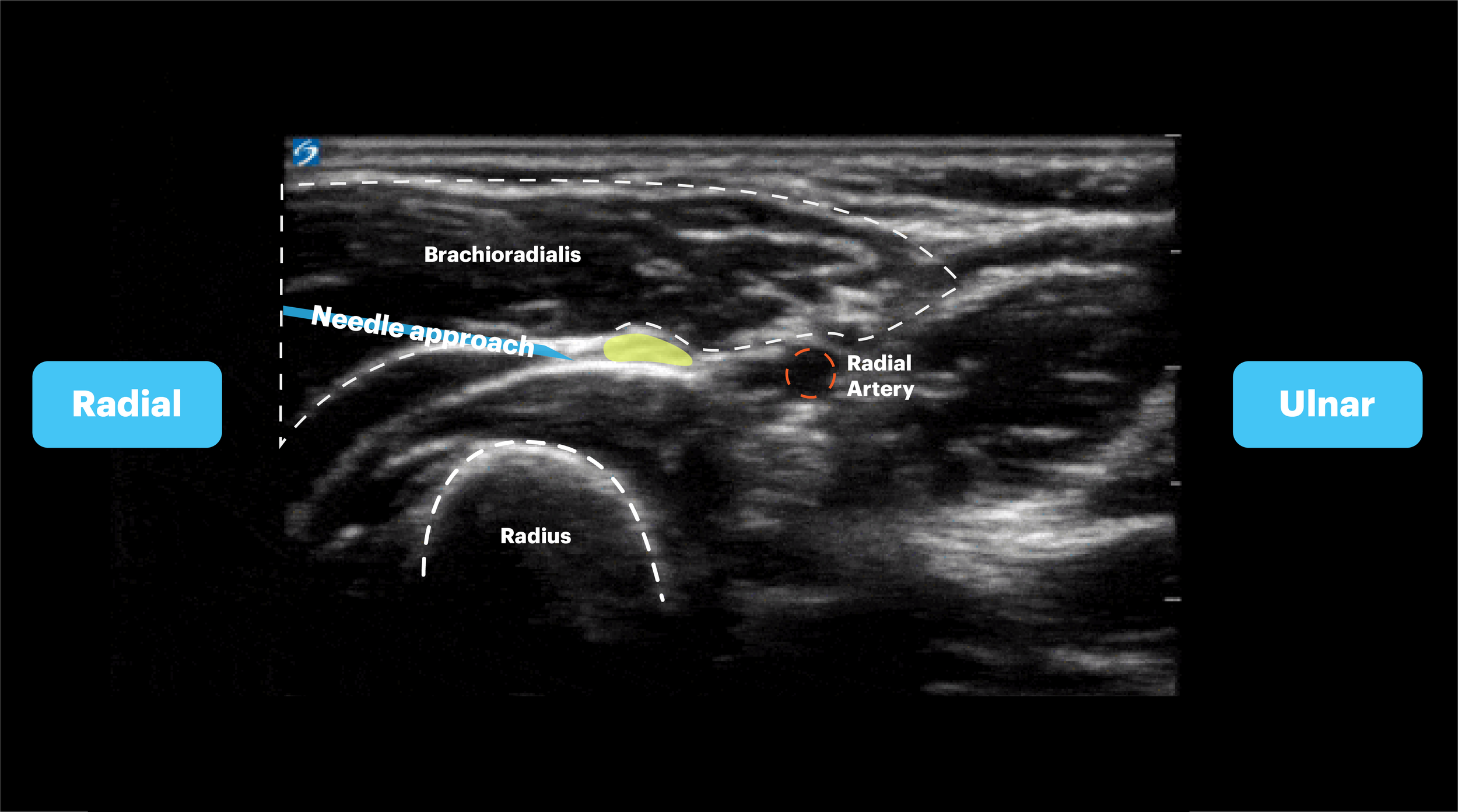
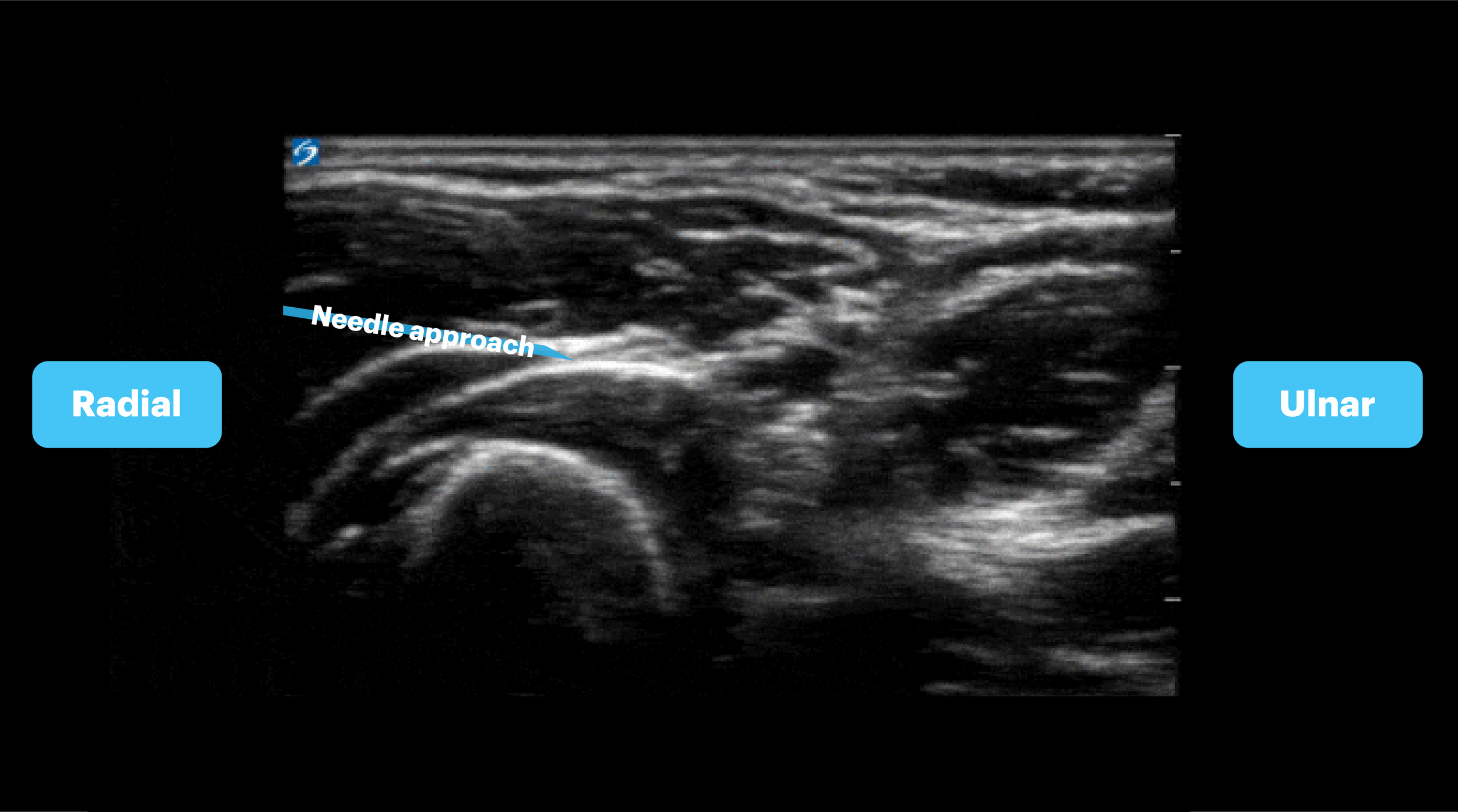
Needle Approach
Our preferred approach is an in-plane technique from the radial aspect of the arm. In this view the radial nerve has now split away from the radial artery and can be seen below the brachioradialis muscle. The nerve is surrounded by fascia on both sides at this point. Advance the needle from a radial to ulnar direction towards the fascial plane surrounding the nerve. You are aiming just adjacent to the nerve to get into the fascial planes, don’t hit the nerve!

Positioning - Elbow
With the arm extended or held over abdomen with elbow flexed, place linear probe in transversely 4-5 cm proximal to the elbow, at the posterolateral aspect. Identify the radial nerve adjacent to the humerus laterally, between the brachioradialis and brachialis muscles. Verify that the nerve does not lie in close proximity to the brachial artery, as this may be the median nerve.
Target Identification
Place the probe in a transverse orientation along the anterolateral aspect of the upper arm, approximately 3-4 cm above the elbow crease. You may immediately identify the hyperechoic radial nerve running in the fascia plane between two muscles (brachioradialis and the brachialis). If not, slide the probe proximally to look for a hyperechoic structure diving deep and posteriorly towards the humerus and into the spiral groove. This is the radial nerve. Once you identify the nerve you can then follow the nerve back distally to find an approachable location to perform the block.
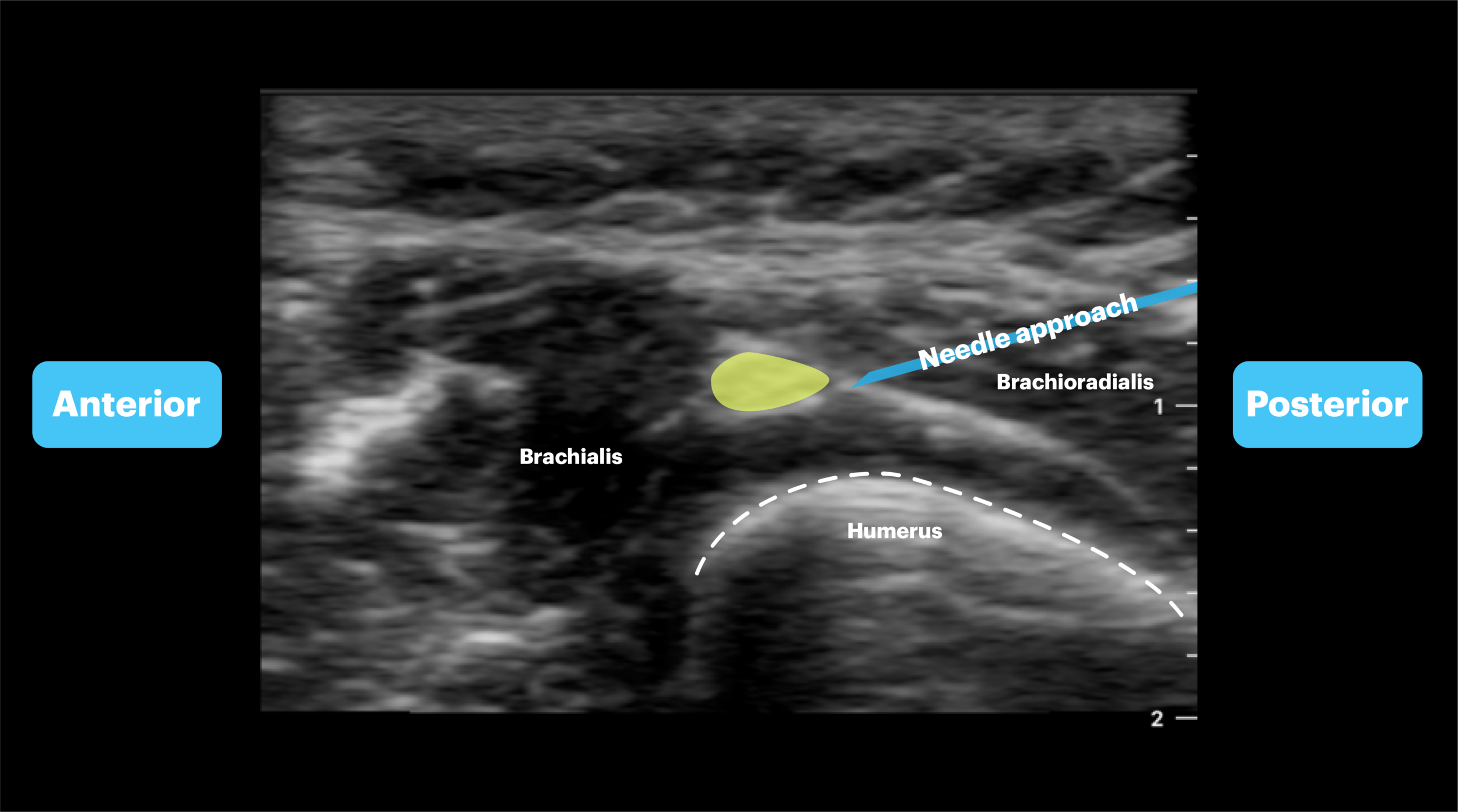
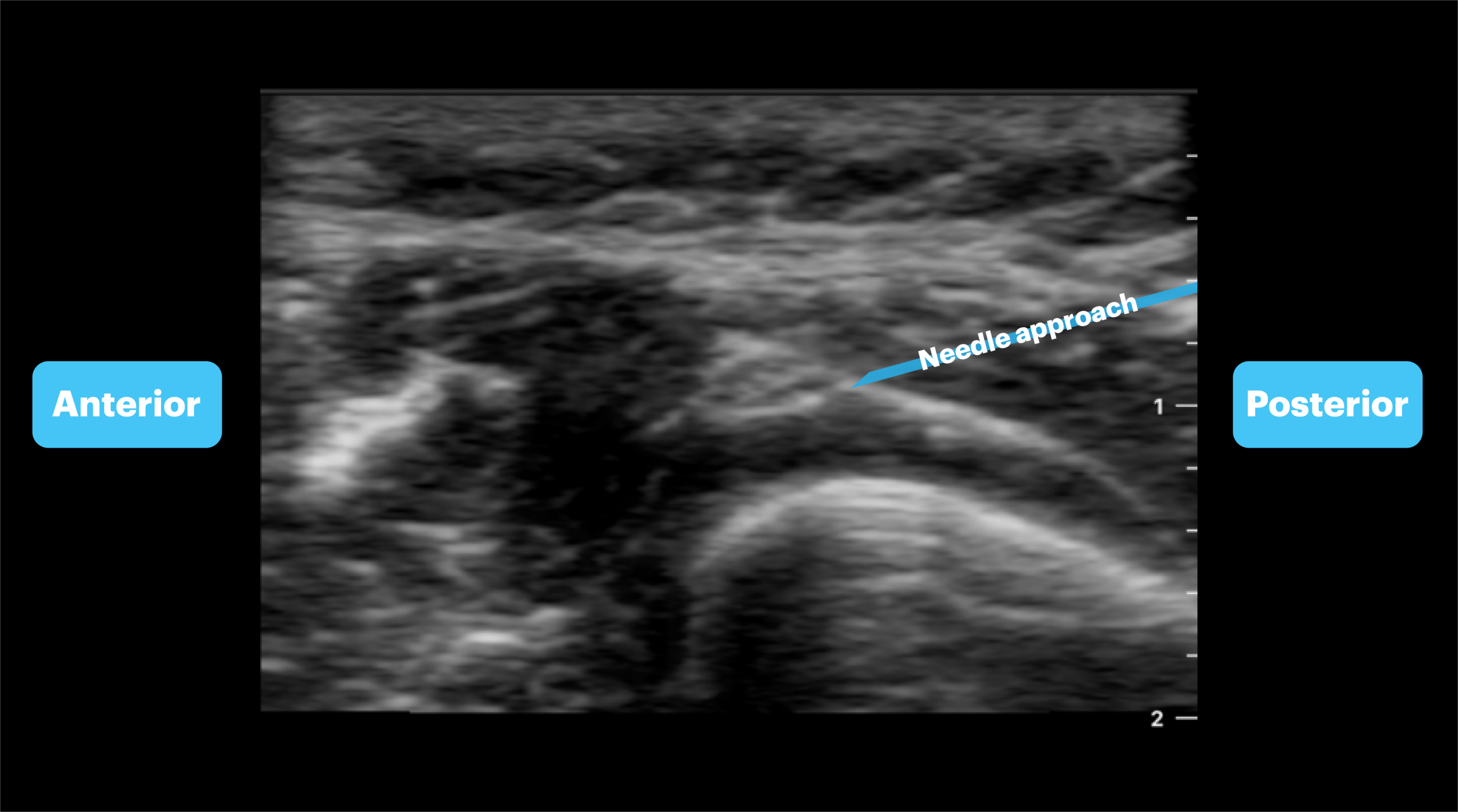
Needle Approach
Use an in-plane technique from an anatomic posterior to anterior direction. In this view the radial nerve can be seen lying in the fascia plane between the brachialis and brachioradialis muscles. The humerus can be seen deep to the muscles. Advance the needle towards the fascial plane surrounding the nerve. You are aiming just adjacent to the nerve to get into the fascial planes, don’t hit the nerve!
Radial Nerve Blocks
Ulnar Nerve Block
Indications: Boxer’s fractures, lacerations, and deep abscesses


Considerations & Technical Details
Considerations:
As the ulnar nerve runs in close proximity to the artery at the wrist, a negative aspiration prior to injection is essential to avoid inadvertent intravascular injection.
Transducer: High-frequency linear probe
Needle: 25-27g 1-1.5 in (2.5-3.8 cm) needle
Anesthetic Volume: 4-5 mL
Target of Anesthetic: Anesthetic spread around the ulnar nerve.
Positioning - Wrist
Position the forearm abducted from the patient, supinated. Place the probe transversely 3-4cm proximal to the wrist. Immediately ulnar to the artery will be the ulnar nerve. If the artery and nerve are too close, trace proximally to separate the nerve from the artery.
Positioning - Elbow
Position the patient with the arm extended, or with the forearm across the patient’s abdomen, with elbow flexed to 90 degrees. Place the transducer transversely 2-3cm proximal to the elbow at the medial of the upper arm. The ulnar nerve is seen superficial to the triceps muscle and typically does not accompany an artery, in contrast to the median nerve.